Anxiety After Illness or Surgery | Marc Cooper Hypnosis
Anxiety after illness or surgery is common, persistent, and often misunderstood. Learn what drives it and why conventional approaches frequently fall short.
ANXIETY
Marc Cooper
5/18/20265 min read
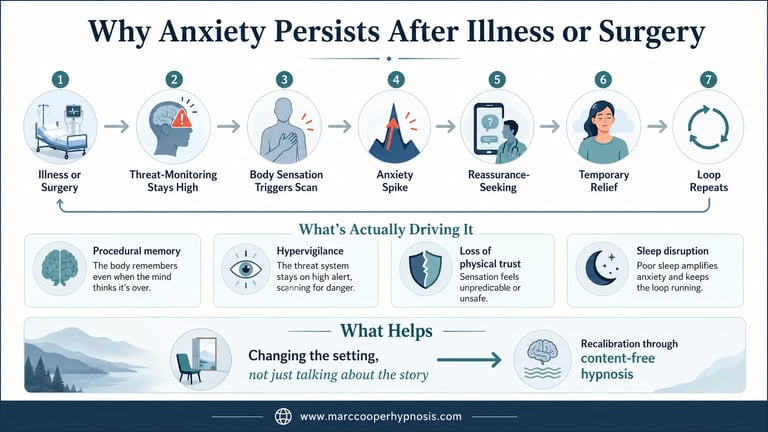
Anxiety After Illness or Surgery: Why It Persists and What's Actually Driving It
Anxiety after illness or surgery is not a personality flaw. It's a pattern. The body went through something real, and the system that monitors threat did not simply reset when the crisis passed.
Most people expect to feel better once the medical part is over. The procedure goes well. The test results are clear. Recovery begins. And yet anxiety remains, sometimes intensifies. That gap between physical resolution and psychological resolution is what this article addresses.
Why Anxiety Persists After Medical Events
The nervous system does not distinguish cleanly between physical danger and anticipated danger. During a serious illness or surgical procedure, the threat-monitoring system is running at high output. It tracks symptoms, outcomes, pain signals, and uncertainty simultaneously.
Once the immediate crisis ends, that system does not automatically downregulate.
It continues scanning. It looks for evidence that the threat is still present. Research has shown that pre-operative anxiety predicts post-operative anxiety, with patients who experienced high levels of anxiety before surgery continuing to feel anxious afterward. In other words, the elevated state becomes a baseline, not an event.
This is not psychological weakness. It's procedural memory. The system learned to treat the body as a source of threat. That learning persists.
There is a second driver that is less frequently discussed. After serious illness or surgery, the person's sense of physical reliability changes. The body did something unexpected. It got sick. It needed repair. That shift in perceived reliability creates a monitoring habit that can outlast the original event by months or years.
How This Shows Up Day to Day
People often notice it in specific, repeatable moments rather than as a constant state.
A physical sensation triggers a scan. A headache registers differently than it did before the illness. A brief shortness of breath after walking upstairs produces a spike of concern that wouldn't have existed previously. What most people normally perceive as ordinary physical discomfort may be experienced with significant anxiety, taken as confirmation of an underlying fear about being ill.
The scan becomes automatic. It runs without permission.
This usually feels like hypervigilance with a medical focus. The person is not generally anxious in the clinical sense. They function. They go to work. They maintain relationships. But part of their attention is perpetually allocated to monitoring the body for signs of recurrence or new danger.
Sleep is often the first casualty. The body relaxes, vigilance drops, and the monitoring system interprets that drop as an opportunity to surface unresolved material. People report lying awake cataloguing physical sensations that they couldn't think clearly about during the day.
Another pattern: reassurance-seeking. Medical appointments, symptom searches, conversations with family members about physical complaints. Reassurance-seeking is only maladaptive if it becomes an enduring and cyclical coping pattern, where patients report symptoms, medical reassurance follows, then a transient fall in anxiety, followed by rapid return of anxiety, sometimes increased. The relief never holds. The loop continues.
Why Talking About It Often Doesn't Resolve It
Understanding why the anxiety is there does not remove it.
A person can correctly identify that their scan is driven by fear, recognize the cognitive distortion, and understand intellectually that their body is functioning normally. They can articulate all of this clearly. The monitoring continues anyway.
This is because the pattern is not primarily cognitive. It runs at a procedural level. It was encoded during an experience of genuine threat, and it does not respond to reasoning the way a belief does. Insight reaches the narrative layer. The pattern runs underneath.
Talk-based approaches often stall here. They can build understanding, reduce shame, and provide context. What they cannot reliably do is access and alter the procedural memory that generates the anxiety response in the first place.
The pattern is not a story. It's a setting.
What a Content-Free Orientation Addresses
When the pattern is procedural rather than narrative, the most efficient point of intervention is the level where the pattern operates.
A content-free approach to this kind of anxiety does not require the person to revisit the details of the illness, reconstruct the surgical experience, or identify the specific thoughts that precede the scan. The content, the story, the narrative of what happened, is not where the pattern lives.
What matters is the system's current configuration. The threat-monitoring is set too high. It was appropriate during the acute event. It has not recalibrated to the post-event reality.
You can read more about how this kind of work is structured in the content-free hypnosis guide.
The work is not about relaxation. It is not about processing trauma in the conventional sense. It is about changing the setting that runs the anxiety, not the content of what the anxiety is about.
Specific Patterns Worth Recognizing
The diagnostic loop. The person feels a symptom, searches it online, finds a possible serious explanation, feels anxiety spike, seeks reassurance, gets temporary relief, and repeats the cycle within days. The loop is self-reinforcing. Each pass through it strengthens the monitoring habit.
Anniversary activation. Anxiety increases in the period leading up to a follow-up scan, a surgical anniversary, or a seasonal marker tied to when the illness began. The system has encoded time-based cues in addition to symptom-based ones. The calendar becomes a trigger.
Functional contraction. The person stops certain activities not because they physically cannot do them, but because those activities now produce anxiety. Exercise, travel, being far from medical care, eating certain foods. The behavioral range contracts around the threat-monitoring system's outputs.
Identity disruption. Pre-illness, the person operated with a background assumption that the body was reliable. Post-illness, that assumption is gone. This is not easily addressed through cognitive reframing because it was not a cognitive belief to begin with. It was an implicit operational assumption. Losing it changes how the person navigates daily life.
What Happens When the Pattern Is Left Unaddressed
Anxiety after illness or surgery tends to either resolve naturally within a few months or chronify.
When it chronifies, the monitoring system becomes increasingly sensitive over time. The threshold for triggering the scan lowers. Activities become associated with risk. The functional range contracts further. Social engagement decreases as the person organizes more of their life around managing the anxiety.
Secondary effects accumulate. Sleep disruption compounds vigilance. Behavioral restriction confirms the implicit belief that the body is unreliable. The person's quality of life narrows without any corresponding change in their actual medical status.
This is not a psychological crisis. Most people who experience it continue to function. But they function at a reduced baseline, and the gap between where they are and where they could be widens with time.
Anxiety following a trauma or medical event tends to respond better to intervention earlier. The longer the pattern runs, the more thoroughly it becomes integrated into the person's behavioral and perceptual habits.
FAQ
Is it normal to feel anxious after surgery or a serious illness?
It is common. Research consistently documents anxiety as a feature of post-surgical recovery and post-illness adjustment. Whether it is temporary or persistent depends on a range of individual factors. The fact that it is common does not mean it resolves on its own.
Why does my anxiety focus on physical symptoms rather than general worry?
Because the original event was physical. The threat-monitoring system learned to treat the body as the primary source of danger. That focus is a logical output of the encoding, not a separate psychological condition.
Why doesn't reassurance from my doctor make the anxiety go away permanently?
Reassurance operates at the cognitive level. The pattern generating the anxiety is procedural. The relief is real but temporary because the underlying setting does not change in response to information.
Can this anxiety appear months or years after the illness or surgery?
Yes. The pattern can remain dormant and activate in response to physical sensations, anniversary dates, medical appointments, or news about illness in others. Delayed onset is common and well-documented.
Will I always have this level of health anxiety after what I went through?
Not necessarily. The pattern is learned, which means it can be changed. The system's current configuration is a response to an event, not a permanent characteristic. When the right kind of intervention reaches the procedural level, the configuration can shift.
When the pattern is running, and insight alone hasn't moved it, that's the work I do.
This article is informational only and not medical or psychological advice.
Address
Based in Los Angeles, CA
Online sessions available worldwide
Contacts

